Background
Restoring a functional level of vision to people who are blind has been a dream of medicine for centuries. Although we are still far from restoration of high-resolution vision, bionic eye technologies are overcoming crucial bottlenecks and are slowly moving from the laboratory into the clinic and onto the free market.
History of Bionic Vision
Advances in medicine, surgery and electronics have set the stage for a fusion of the physical and biological sciences; one in which visual prostheses may restore lost functional capacity to the disabled. For excellent reviews on the subject, see [1, 2, 3].
The Early Days
The end of the 18th century saw the introduction of electrophysiology as a scientific discipline, opening the door to many studies of cortical stimulation.
1752
Benjamin Franklin theorized to the Royal Society of London that sight and hearing could be restored with the use of electricity [4].
1755
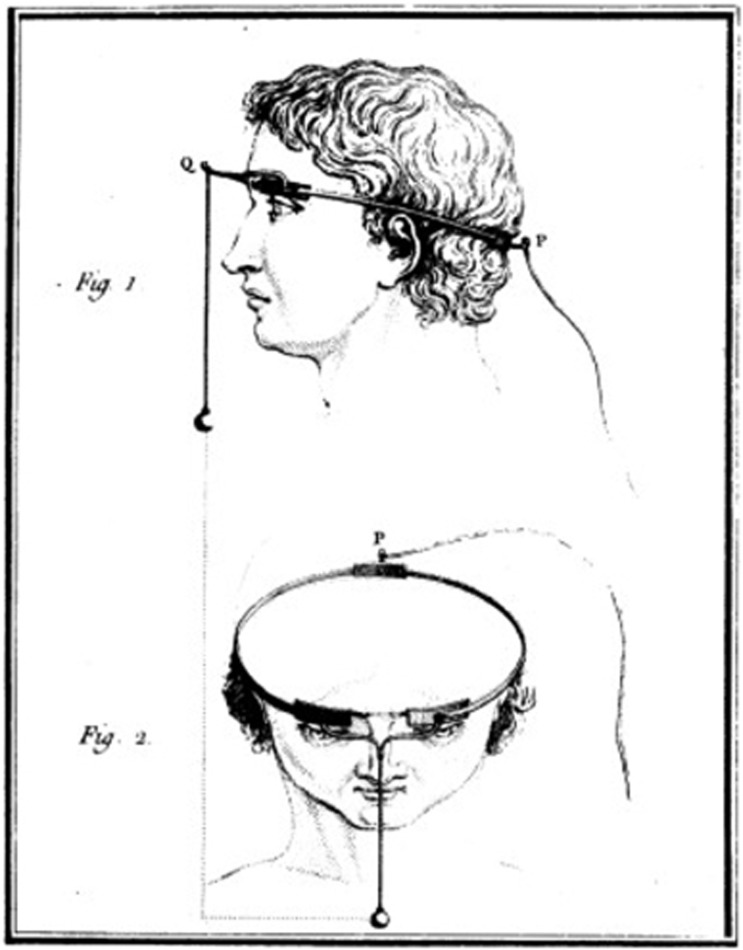
Charles Le Roy, an 18th century French scientist, conducted the first attempt to cure blindness through electrical stimulation (presumably after reading Benjamin Franklin's theory). Le Roy was able to evoke flashes of light (phosphenes) and other visual disturbances in a blind patient by sending electrical currents through a wire wrapped around the patient's head [5].
Fig. 1: Method used by Charles Le Roy to evoke visual disturbances in a blind volunteer. A wire was wrapped around the patient's head with current applied through it. (reproduced with permission from [6])
1870
Two German physicists called Gustav Theodor Fritsch and Eduard Hitzig performed a number of experiments involving systemic stimulation across the cerebral hemispheres of dogs. These studies demonstrated that cerebral hemispheres were excitable at a time when many scientists believed that they were not [7].
1884
Victor Horsley, a British scientist, is credited as the first to use electrical stimulation of thecerebral cortexintraoperatively. Horsley electrically stimulated an occipital encephalocele in a 6-week old child [8], in response to which the child's eyes showed rapid conjugate deviations.
Treatment of Head Injuries in the World War Era
The beginning of the 20th century saw the introduction of cortical stimulation as a treatment option for epilepsy. With the increased occurrence of gunshot and battlefield wounds to the head, neurosurgeons reported a wide variety of phosphenes in response to cortical stimulation.
1918
Kurt Löwenstein & Moritz Borchardt electrically stimulated the exposed visual cortex of a patient who suffered persistent seizures from a bullet wound on the left side of his head. The stimulation produced flickers of light that closely resembled the visual phenomena the patient would see preceding a seizure, showing that stimulation of the visual cortex could produce point sources of light [9].
1924
Fedor Krause introduced surgical operations for treatment of epilepsy in Germany, performing over 400 operations on epileptic patients. When he stimulated the cortex of a gunshot wound victim, the patient reported seeing jagged rings of light and stars in different patterns. Krause observed that even though his patient washemianopicfor nine years, he still experienced visual hallucinations in his blind hemifield preceding a seizure. Electrical stimulation could provoke similar visual imagery in the blind hemifield as well [10].
1929
Otfried Förster, a German neurologist and neurosurgeon, examined a patient with a projectile injury that resulted in occipital seizures. He demonstrated that stimulation of theoccipital poleand its surrounding cortex produced phosphenes that were motionless and located at the center of the patient’s visual field [2].
1947
The American-Canadian neurosurgeon Wilder Graves Penfield examined 17 years of visual cortex stimulation in about 330 operations. He stimulated a wide area of the visual cortex and also one area outside the occipital lobe, which still produced visual imagery. The observations of Penfield were unique in that patients reported seeing phosphenes of different colors [11].
The First Generation of "Bionic Vision" Implants
By the 1950s, it was well known that electrical stimulation of the occipital poles could produce punctate phosphenes in the centre of the visual field [3]. This knowledge, plus Krause's observation that it was possible for a blind patient to perceive visual imagery upon stimulation of the occipital cortex, prompted the suggestion that a visual prosthesis might be a practical possibility.
1962
"I see a flash!" - Button (1958, p.54)
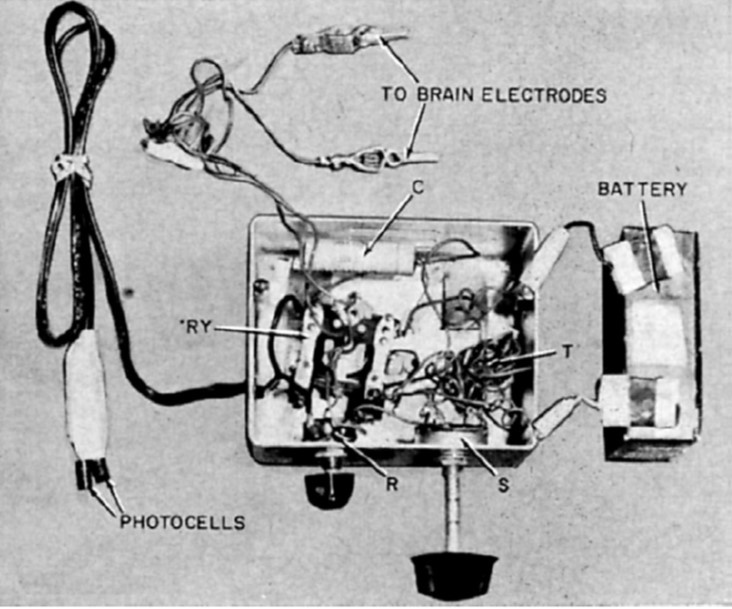
John C. Button and Tracey Putnam at Cedars of Lebanon Hospital (now Cedars-Sinai) in Los Angeles created and implanted the first ever bionic vision device in a 36-year old woman who had been completely blind for 18 years. Two pairs of stainless steel wires were implanted into the cortex and connected to a simple stimulator. The patient reported seeing vivid flashes of light and (with the use of a photocell) was able to detect the presence and relative brightness of a light source [3].
Fig. 2: Button's stimulating apparatus was connected to an array of four stainless steel wires implanted in the occipital cortex of a blind woman. (reproduced under CC BY-NC-ND 4.0 from [2])
1965
Giles Brindley, a physiologist at the University of Cambridge, had been undertaking a programme of research to support the development of a fully implanted, multielectrode wireless visual cortex stimulation device developed a fully implanted, multielectrode, wireless visual cortex stimulation device with the goal of allowing prosthesis recipients to read printed or handwritten text [5].
1966
The first Conference on Visual Prosthesis was held in Endicott House at the Massachusetts Institute of Technology. The conference chair Theodore Sterling explained that after initial difficulty in bringing together potential participants, the conference was finally held under the proviso that the proceedings would not be made publicly accessible [2].
1968
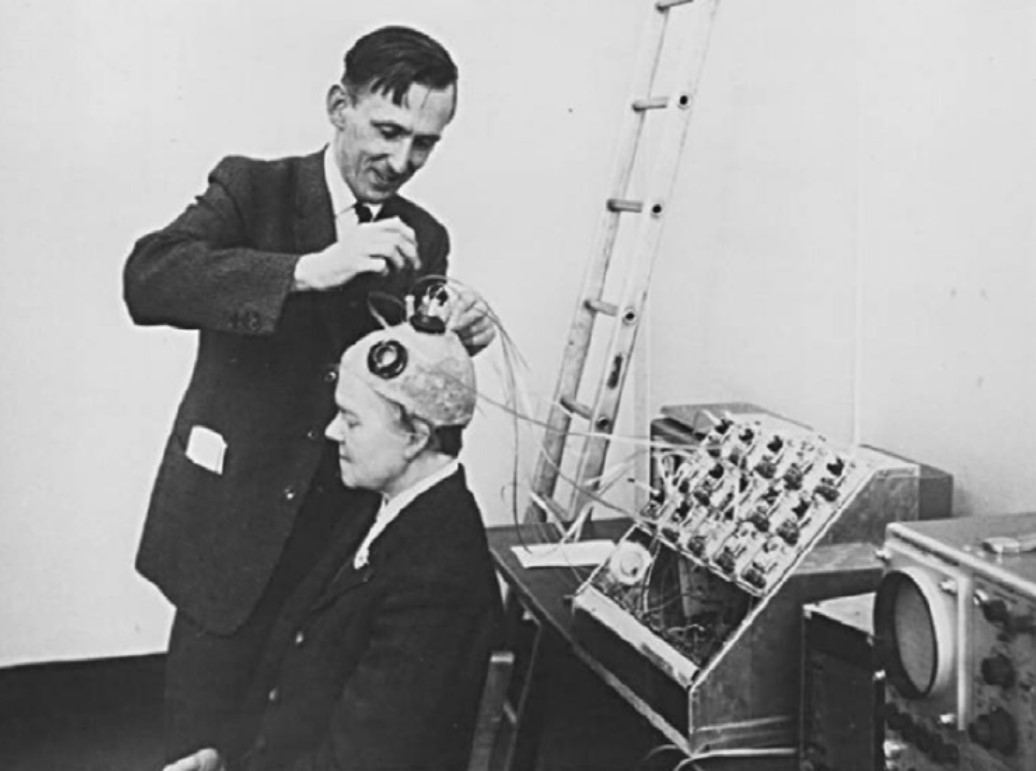
Brindley and Lewin implanted their first cortical implant that consisted of an array of 80 small, square, platinum electrodes embedded in a silicone cap. Each electrode was hard-wired to a receiving coil that was part of an array of coils also embedded in silicone and implanted under the scalp. 39 electrodes in the implant produced phosphenes across the patient’s visual field when stimulated. Centrally evoked phosphenes were small and flickering whereas peripherally evoked phosphenes differed more in size, shape, brightness, and sharpness [12].
Fig. 3: Brindley stimulating the visual cortex of his first implant recipient, placing a stimulating coil over a matched receiving coil implanted under her scalp. (reproduced under CC BY-NC-ND 4.0 from [2])
The Era of Government-Funded Research
The same year that Brindley & Lewin published their groundbreaking paper, the UK Medical Research Council formed the Neurological Prosthesis Unit, with Brindley as its director. In the US, the University of Utah instigated a sensory prosthesis research program with William Dobelle as director. In addition, the National Institute of Health (NIH) established a neuroprosthetic program at the US National Institute of Neurological Diseases and Blindness (NINDB, now known as NINDS). Thus began the era of government-funded research towards the development of a cortical visual prosthesis:
1969
The second Conference on Visual Prosthesis was held at the University of Chicago, aimed at trying to find future directions necessary to explore a possible visual prosthesis [2].
1974
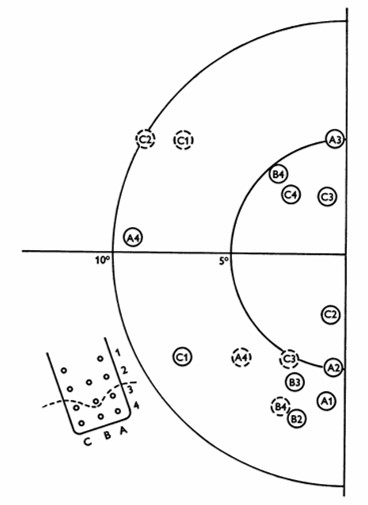
William Dobelle and his group developed a removable multielectrode cortical surface array, which was tested on 36 sighted patients undergoing occipital surgery [13] and 2 blind volunteers who had been blind for 7 and 28 years, respectively [14]. The array contained 64 hexagonally arranged platinum discs placed only over the mesial occipital cortex, each of 1-mm2 surface area. Their results in blind subject closely agreed with Brindley & Lewin's [12], noting that phosphenes could be elicited with stimulation of V2 and persisted with suprathreshold stimulation. The same was not true in sighted volunteers, where phosphenes did not always flicker and were occasionally coloured, always disappeared immediately upon cessation of stimulus, and gradually faded with continuous pulse trains [13].
Fig. 4: Phosphene map in the visual field for case no. 36. Phosphenes indicated by dashed circles appear only at high amplitudes. The electrode array and numbering system are also shown, along with a dashed line showing the postulated position of the calcarine fissure. (reproduced with permission from [14]).
1974
Over the same period, researchers from the Huntington Institute of Applied Medical Research also developed and tested a cortical array comprising smaller, "strip" arrays of 18 platinum surface electrodes, placed separately on both the occipital pole and mesial occipital cortex of normally sighted patients [2, 15]. The implant was able to elicit phosphenes, but could also cause seizures, which led the NIH to disbandon the group's effort in favor of research on "safe and effective methods for neural stimulation" [2].
1975
Another group funded by the NIH and based at the Massachusetts General Hospital in Boston had been undertaking intraoperative visual cortex stimulations on five patients throughout the early 1970s. However, only three patients reported seeing phosphenes, with the two failures attributed to postoperative swelling and patient drowsiness [2].
1978
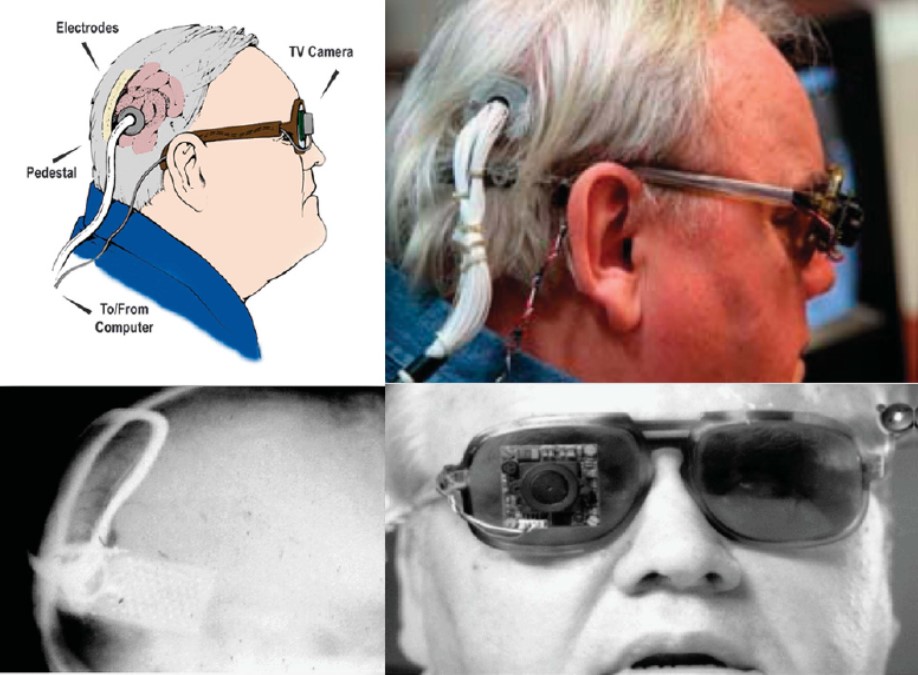
Dobelle and colleagues continued to improve their implant design throughout the 1970s, adding a transcutaneous connector to permit chronic implantation of electrodes and spectacle-mounted cameras. One of Dobelle's early patients retained his implant for over 20 years, with no reported complications of infection or seizure [2].
Fig. 5: Different views of a recipient of the Dobelle implant, first implanted in 1978. In 2000, his external hardware & software was upgraded, including the miniature camera shown, greatly enhancing the functionality of his prosthesis. (reproduced with permission from [6])
1982
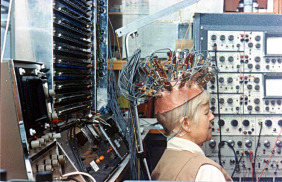
Determined to pursue the goal of reading conventional letterforms, Brindley's group continued developing improved implants into the 1980s including one with 151 electrodes [13], which unfortunately became infected and had to be removed [14].
Fig. 6: "Miss Bonnett", recipient of the last visual cortex implant built by the MRC Neurological Prostheses Unit. (reproduced under CC BY-NC-ND 4.0 from [2])
The Era of Retinal Implants
The considerable risk associated with cortical prostheses led to the scientific community to explore other locations along the visual pathway capable of producing phosphenes, which led to a new era focused on the development of retinal prostheses.
1996
Mark Humayun and colleagues showed that local electrical stimulation of the retinal surface in patients with outer retinal diseases resulted in focal light perception, even though the patients had been blind for many years [16].
2011
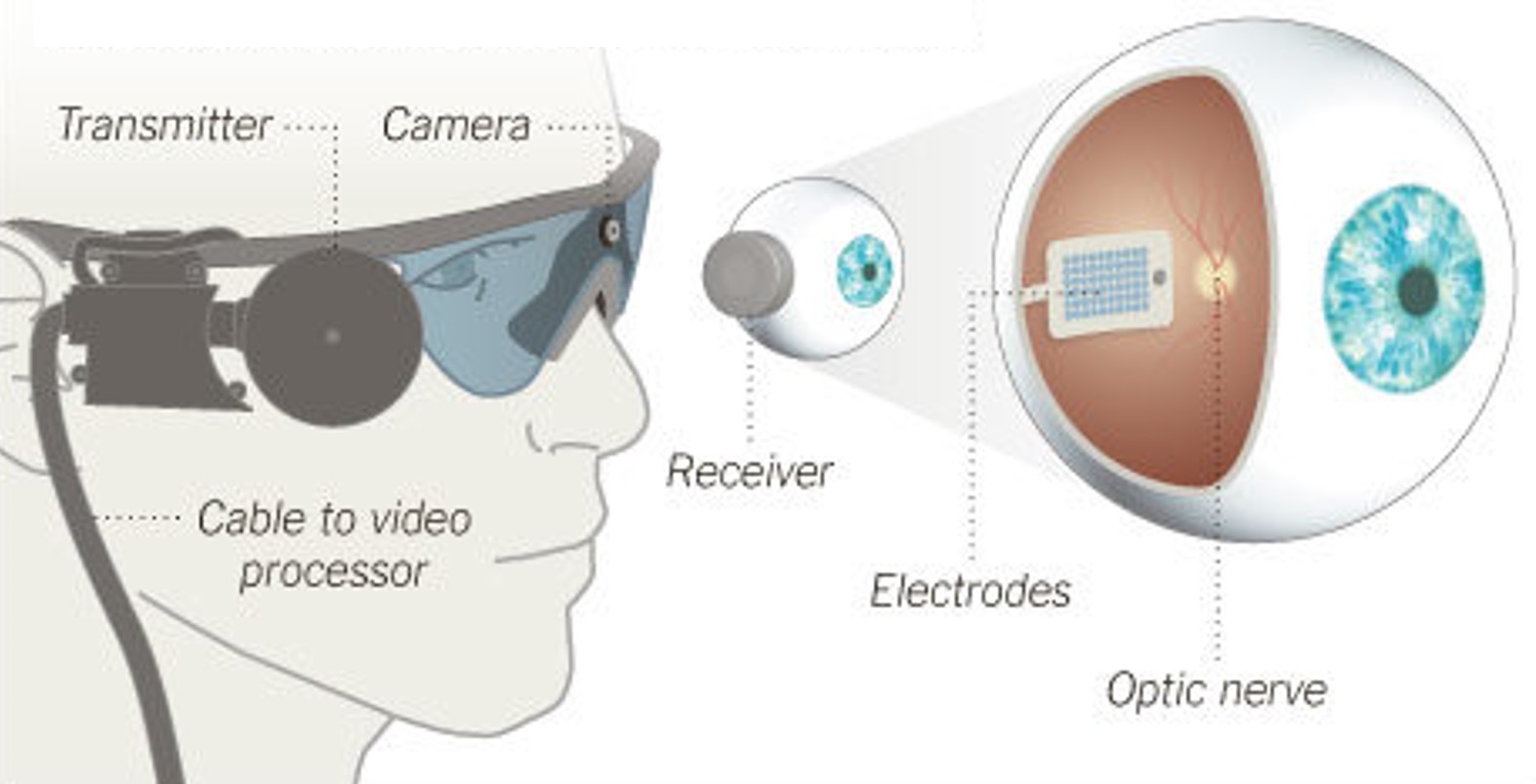
Argus II, anepiretinalimplant developed by Second Sight Medical Products, received approval for commercial use in the European Union (CE Mark). The implant was initially available at a limited number of clinics in Switzerland, France, and the United Kingdom, at an EU market price of $115,000 [17].
Fig. 7: Argus II Retinal Prosthesis System (Source: Second Sight). Camera images are processed and transferred to electrodes implanted in the back of the eye.
2013

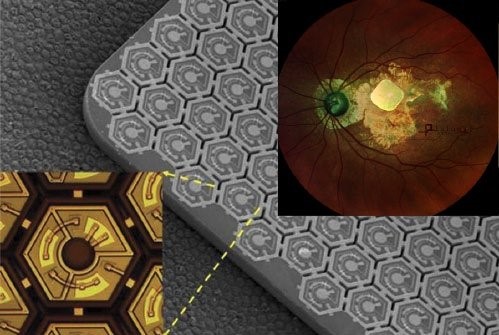
Alpha IMS, asubretinalimplant developed by Retina Implant AG, received the CE Mark as well [18]. The implant was initially available at around $130,000.
Meanwhile in the US, Argus II became the first retinal implant to receive FDA approval [19].
Fig. 8: Alpha IMS, a subretinal implant consisting of a 3x3mm2 microchip with 1,500 electrodes (Source: Retina Implant AG).
2019
Retina Implant AG discontinued business activities quoting innovation-hostile climate of Europe's rigid regulatory and unsatisfactory results in patients.
2020
Stricken by fundraising issues due to COVID-19, Second Sight announced massive lay-offs and an intent to wind down operations. The company would later attempt a (failed) business merger with Pixium Vision but ultimately rebound after raising ~$60M in a public offering.
2021
Pixium Vision implanted their first of an expected 38AMDpatients with PRIMA, a subretinal implant, as part of their PRIMAvera clinical trial. This study is the last step before seeking market approval for dry AMD in Europe.
In addition, Pixium expects to report 36-month data from the French feasibility study by early 2022, and is continuing clinical development in the US.
Fig. 9: PRIMA, a subretinal implant consisting of ~400 photovoltaic cells (Source: Pixium Vision).
The Future
2020s - ?
With dozens of next-generation implants in development that include retinal, optic nerve, and cortical approaches, a wide variety of bionic eye technologies should be available within a decade.
Causes of Vision Loss
Vision loss can occur in a number of ways. The main focus of retinal prosthetic research is to improve functional vision for people with blindness and/or vision impairment from the result of hereditary diseases, such as retinitis pigmentosa (RP) and age-related macular degeneration (AMD).
Disclaimer: The following is for informational purposes only. If you think you are subject to one of the conditions described below, please consult with your care provider.
Retinitis Pigmentosa
Retinitis pigmentosa (RP) is the most common form of inherited blindness that affects 1 in every 3000 – 7000. RP is the result of a change in a gene or genes that would typically lead to functioning photoreceptors, but instead create smaller photoreceptors with a disorderly arrangement. RP develops over a longer period of time compared to other vision diseases, sometimes spanning a person's entire life. Symptoms for RP usually include peripheral vision field loss (also known as "tunnel vision") and night blindness. Currently, there is no known cure for RP.
There are two classifications of RP: syndromic and non-syndromic. Non-syndromic RP is more common than syndromic RP and does not develop with other diseases or disorders. Syndromic RP can occur with other medical conditions or disorders where neurosensory systems other than the eye are affected. People with syndromic RP make up an estimated 20-30% of all RP patients. All RP types are a degradation of the retina caused by genetics, also known as a dystrophy. The rod-cone dystrophy is usually syndromic and involves a loss of cone activation due to relative low rod activation, which present with loss of central vision as well as the usual peripheral vision field loss associated with RP.
RP is associated with a number of different conditions. Usher syndrome, for example, is a combination of RP and deafness and is estimated to contribute to 14% of all RP cases overall. Bardet-Biedl syndrome is a rare genetic disorder that presents with rod-cone dystrophy. Some forms of RP are associated with mitochondrial disorders, such as the Kearns-Sayre syndrome, where the area of the macula is more affected than the periphery.
Implants that may be able to treat RP include Argus II, the suprachoroidal implant, and other retinal implants as well as cortical implants.
Age-Related Macular Degeneration (AMD)
In 2010, there were 2.07 million people with AMD. That number is expected to double to 5.44 million by 2050. As with most health conditions, aging is a significant risk factor for AMD.
The macula is a pigmented circular area located on the back of the eye on the retina. Within the macula is the fovea, an area responsible for processing our central field of view.
There are three factors that are used to characterize the different types of AMD: size of drusen, type of damage caused by progression, and presenting as either “wet” or “dry”. Small yellow deposits of drusen (made of proteins and lipids) can build up in the macula, usually as a sign of Early AMD. Intermediate AMD involves larger size drusen deposits and a change in retinal pigment functioning. While intermediate AMD can cause some vision loss, both early and intermediate AMD are typically present without other symptoms.
Late AMD presents with loss of central vision due to progressive damage to the retina, either as wet AMD or geographic atrophy. Wet AMD, also known as neovascular AMD, is specifically caused by irregular blood vessel growth. These blood vessels can be easily damaged allowing for blood and proteins to spread into the area of the macula. Damage that leads to the degradation of three specific areas of the eye (neighboring photoreceptors, retinal pigment epithelium, and the choriocapillaris) is referred to as geographic atrophy. Further research into how AMD can affect the different layers of the retina is needed to better understand the physiology of geographic atrophy.
Dry AMD includes any type of AMD that is not neovascular or wet. Dry AMD has a significantly higher prevalence of all AMD patients (estimated at 80% or more) compared to Wet AMD.
Implants that may be able to treat AMD include PRIMA as well as other retinal and cortical implants.
Sight Restoration Technologies
Bionic Vision is not limited to computer interfaces but instead encompasses a wide range of vision restoration and/or rehabilitation techniques.
Electronic Neuroprostheses
Neuroprostheses, better known as "implants", have been a common focus of research and investments into curing blindness. These implants come in the form of a miniature chip which is placed into a specific location of the retina (retinal implants) or the brain (cortical implants).
Retinal implants function to replace damaged photoreceptor cell activation. However, if the disease has significantly interrupted the early visual pathway (i.e. the retina, optic nerve, or lateral geniculate nucleus), cortical implants may be the only option.
Optogenetic Neuroprostheses
Optogenetics is a technique that uses a combination of optical and genetic methods to restore vision loss. Once light-sensitive proteins are introduced to the area of the damaged photoreceptors, retinal neurons can be stimulated by using a specific range of light intensities and wavelengths.
Two types of optogenetic strategies have been studied: ion channel therapies and G-protein coupled receptor (GPCRs) therapies. Ion channel therapy research focuses on improving temporal sensitivity for vision. While slower than ion channels, GPCR therapies have demonstrated much promise for vision restoration given their higher sensitivity to light activation. Both have been used to study and treat retinal dystrophies and degenerative diseases.
There are a few companies in the process of developing accurate optogenetic studies for future use. The GenSight PIONEER preliminary trial combines optogenetic therapy with biomimetic goggles. These specially designed goggles help to compensate for spatiotemporally related visual distortions associated with optogenetic treatment.
Gene-Based Therapies
When there is a mutation of a gene, the synthesis of proteins that follows is affected such that there can be an increase or inhibition of function for that gene. Inhibiting the function of a protein within the retina can lead to diseases that cause blindness. Gene therapy and gene editing are two current genetic approaches being studied to prevent the spread of retinal disease and possibly restore vision.
Gene therapy involves using recombinant DNA to encode the desired DNA into a plasmid which is delivered into the cell by a vector. This is meant to cause the expression of the desired gene throughout the retina, and restore cellular function. A limitation of gene therapy is that it can only function to supplement the expression of a gene, not eliminate or suppress the desired genetic expression. There has been significant progress in gene therapy for treating Leber congenital amaurosis, which shows promise in treating more frequent diseases in vision such as AMD and RP.
Cell Therapy
Once they are successfully injected or transplanted into the retina, stem cells have the ability to form all cell types necessary for retinal regeneration. There are two types of stem cells that can do this: embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs). Embryonic stem cells and induced pluripotent stem cells are both pluripotent, meaning that they can develop into many specialized cell types, including retinal cells.
Inserting stem cells within the retina may be conducted through an injection process or a transplantation. There have been multiple trials over the past ten years testing the usefulness of stem cell therapy within the retina, mostly yielding promising results. Research has focused on studying the effectiveness of stem cell therapy in creating retinal pigment epithelium (RPE) cells and photoreceptor cells. Data suggest that iPSC transplants can produce RPE cells and have potential to restore vision or even slow the progression of disease for AMD patients. There are currently no clinical trials that have demonstrated the effectiveness of stem cell therapy for photoreceptor cells.
Sensory Substitution
Sensory substitution devices change visual information to auditory or tactile information. What is most notable about these solutions is that they do not require invasive surgery for use, instead relying on the plasticity of other sensory modalities to adapt new strategies to compensate for vision loss. When paired with extensive training, people who are blind or have low vision can improve performance in navigation, object recognition, and more.
Implants in this category include the vOICE (visual to auditory) and BrainPort (visual to tactile).
Glossary
Action potential
An action potential is a rapid, temporary change in voltage across a neuron's membrane. Once the membrane reaches a threshold, the signal travels along the axon without gradually fading. Action potentials allow neurons to communicate over distance and are often described as neural spikes.
Activities of daily living (ADLs)
Activities of daily living (ADLs) are basic tasks involved in caring for oneself, such as eating, bathing, dressing, toileting, transferring between positions, and moving within the home. Clinical and rehabilitation studies may measure ADL performance to evaluate independence and the practical effects of an intervention.
Adverse event
An adverse event is an undesirable medical occurrence in a participant receiving a treatment or taking part in a clinical study. It does not necessarily mean that the treatment or device caused the event. Researchers record severity, timing, outcome, and whether the event may be related to the intervention.
Age-related macular degeneration (AMD or ARMD)
Age-related macular degeneration (AMD) is a disease that damages the macula, the central part of the retina responsible for detailed vision. It can cause distortion, blurred central vision, or a central blind spot, while peripheral vision is often preserved. AMD occurs in dry and wet forms and is a major cause of vision loss in older adults.
Biocompatibility
Biocompatibility is the ability of a material or device to perform its intended function without causing an unacceptable response in the body. For a neural implant, relevant responses include inflammation, toxicity, fibrosis, tissue damage, and changes at the electrode-tissue interface.
Biological realism
Biological realism describes how closely a model or simulation reflects known biological structure, mechanisms, or behavior. A model can be biologically realistic at one level, such as cell shape, while simplifying another, such as molecular signaling. More realism is not always better; the appropriate level depends on the question being studied.
Biphasic pulse
A biphasic pulse has two phases with opposite electrical polarity. Neural stimulators commonly use biphasic waveforms so that charge delivered in one phase is partly or fully reversed in the other, reducing net charge left at the electrode-tissue interface.
Bipolar cell
A bipolar cell is a retinal neuron that receives input from rods or cones and passes signals toward retinal ganglion cells. Different bipolar-cell types separate visual information into parallel pathways, including responses to increases or decreases in light. Some sight-restoration approaches target bipolar cells because they may survive after photoreceptors degenerate.
Blindness
Blindness refers to severe vision loss. It does not necessarily mean a complete absence of sight; many blind people retain light perception or some usable vision. Depending on the context, blind may describe a clinical or legal category, a functional experience, or a personal identity. Some people capitalize Blind when referring to a shared cultural identity or community.
CE marking (Conformité Européenne)
CE marking, from the French Conformité Européenne, indicates that a product conforms to applicable European requirements and may be placed on the relevant European market. For medical devices, the manufacturer completes a conformity assessment and issues an EU declaration of conformity; higher-risk devices generally also require assessment by an independent notified body. The phrase CE approval is commonly used but is technically imprecise, because the CE mark is not an approval issued by a single European regulatory agency.
Cataract
A cataract is a clouding of the normally clear lens inside the eye. It can cause blurred or dim vision, glare, halos around lights, reduced color perception, and difficulty seeing at night. Cataracts often develop gradually and can usually be treated by replacing the cloudy lens with an artificial one.
Cell morphology
Cell morphology describes a cell's shape and structural features, including the size of its cell body and the arrangement of its processes. For neurons, morphology can influence which cells they connect with and how they respond to electrical stimulation.
Cell therapy
Cell therapy uses living cells to replace lost cells, repair tissue, or support cells that remain. In sight restoration, researchers are studying transplantation of retinal pigment epithelial cells, photoreceptor precursors, and other retinal cells. The transplanted cells must survive, integrate safely, and provide a useful function.
Cerebral cortex
The cerebral cortex is the folded outer layer of the cerebrum. Different cortical regions contribute to sensory perception, movement, language, memory, and other higher functions. The visual cortex occupies part of the cerebral cortex at the back of the brain.
Channelrhodopsin
Channelrhodopsin is a light-sensitive protein originally found in algae. When expressed in a cell, it opens in response to particular wavelengths of light and allows ions to cross the cell membrane, typically increasing electrical activity. Channelrhodopsins are widely used in optogenetics and are being studied as a way to make surviving retinal neurons light-sensitive after photoreceptors have been lost.
Charge density
Charge density is the electric charge delivered through an electrode divided by the electrode area, often reported per stimulation phase. It helps compare stimulation across electrodes of different sizes and is an important consideration for both neural activation and electrode-tissue safety.
Clinical intervention
A clinical intervention is an action intended to prevent, diagnose, treat, or manage a health condition. It may involve a drug, device, surgery, therapy, behavioral program, or other form of care. In a clinical study, an intervention is evaluated using predefined safety and outcome measures.
Clinical trial
A clinical trial is a prospective research study in human participants that evaluates a medical intervention, such as a drug, device, surgery, or rehabilitation program. Trials follow a predefined protocol and may assess safety, feasibility, effectiveness, or other outcomes. They require ethical review and informed consent.
Cone photoreceptor
A cone photoreceptor is a light-sensitive retinal cell that supports color vision and fine spatial detail, especially in daylight. Cones are concentrated in the macula and packed most densely in the fovea. Loss of cones can severely impair central vision, reading, and face recognition.
Congenitally blind
Congenital blindness is blindness or severe vision loss that is present from birth. It can result from genetic conditions, differences in eye development, infection, or injury before or around birth. The term describes when the vision loss began, not its cause or the amount of residual vision.
Contrast sensitivity
Contrast sensitivity is the ability to detect differences in brightness between an object and its background. It is commonly measured across a range of spatial frequencies because vision may be more sensitive to some pattern sizes than others. A person can have relatively good visual acuity but still have poor contrast sensitivity.
Cortical plasticity
Cortical plasticity is the ability of the cerebral cortex to change its activity, connections, or functional organization. These changes can occur during development, learning, sensory loss, rehabilitation, or exposure to restored or artificial sensory input. Plasticity may support adaptation to a visual prosthesis, although its extent and functional effects vary across individuals and circumstances.
Cortical prosthesis
A cortical prosthesis is a neuroprosthesis that interfaces directly with the cerebral cortex. For vision restoration, electrodes stimulate visual cortex to create percepts while bypassing the eyes and optic nerves. The electrodes may rest on the cortical surface or penetrate into the tissue, depending on the design.
Cortical stimulation
Cortical stimulation is the application of electrical, magnetic, or other stimulation to the cerebral cortex. In visual prostheses, electrical stimulation of visual cortex can evoke phosphenes by activating neurons that normally process visual information. The resulting percept depends on factors including the stimulation location, electrode design, current, and timing.
Cortical surface implant
A cortical surface implant places electrodes on the outer surface of the cerebral cortex rather than inserting them into the tissue. Surface electrodes can stimulate or record from relatively broad regions while generally causing less direct tissue injury than penetrating electrodes. Their greater distance from individual neurons may limit the spatial precision of stimulation.
Coulomb
The coulomb is the SI unit of electric charge. One coulomb is the amount of charge transferred by a current of one ampere in one second. Neural stimulation pulses usually deliver much smaller amounts, often reported in nanocoulombs or picocoulombs.
Defense Advanced Research Projects Agency (DARPA)
The Defense Advanced Research Projects Agency (DARPA) is a research and development agency of the U.S. Department of Defense. It funds ambitious, often early-stage projects intended to create major technological advances, including work in neuroscience, neural interfaces, and medical devices.
Diabetic retinopathy
Diabetic retinopathy is damage to the retina caused by diabetes. Changes to retinal blood vessels can lead to leakage, swelling, poor blood supply, or abnormal new vessel growth. The disease may initially have few symptoms but can cause blurred vision, floaters, or severe vision loss; regular screening can detect it before vision is affected.
Early feasibility study (EFS)
An early feasibility study (EFS) is a limited clinical investigation of a medical device early in its development. It typically enrolls a small number of participants to evaluate initial clinical safety, device functionality, and the basic design concept. Results may be used to refine the device or study procedures before larger trials.
Electrical stimulation
Electrical stimulation uses controlled electric current to alter the activity of excitable cells such as neurons. In a visual prosthesis, current delivered through an electrode can activate nearby cells and evoke a phosphene. Its effects depend on parameters including current amplitude, pulse width, waveform, and stimulation frequency.
Electrode impedance
Electrode impedance describes how strongly an electrode and the surrounding interface oppose an alternating electrical current. It depends on frequency, electrode material and area, tissue properties, and the condition of the interface. Impedance affects the voltage needed for stimulation and the quality of recorded neural signals.
Electrode-neuron coupling
Electrode-neuron coupling describes how effectively and selectively an electrode interacts with nearby neurons. It depends on factors such as distance, tissue properties, electrode geometry, cell orientation, and the stimulation or recording method. Strong or stable coupling can lower stimulation thresholds and improve recordings, while changes in coupling can alter implant performance.
Electrophysiology
Electrophysiology is the study of electrical activity in biological cells and tissues. In neuroscience, it includes recording voltages or currents from ion channels, individual neurons, neural populations, or larger structures. Electrical stimulation may also be used to test how cells and circuits respond.
Encapsulation
Encapsulation is the formation of a layer or capsule of tissue around an implanted material. It is part of the body's foreign-body response and may help isolate the implant. A thick fibrous capsule can also increase the distance between an electrode and neurons or otherwise alter device performance.
Encephalocele
An encephalocele is a condition in which brain tissue, its protective membranes, or both protrude through an opening in the skull. It develops before birth when part of the skull does not close completely. Its effects depend on the location, size, and amount of neural tissue involved.
Epiretinal
Epiretinal means located on the inner surface of the retina, next to the vitreous and close to retinal ganglion cells. An epiretinal prosthesis places electrodes in this location to stimulate ganglion cells or their axons, bypassing damaged photoreceptors and much of the remaining retinal circuitry.
Ex vivo
Ex vivo describes experiments performed on organs, tissue, or cells that have been removed from an organism and studied outside the body. The sample is often kept viable so that some of its original structure and function are preserved.
Fibrosis
Fibrosis is the excessive formation of fibrous connective tissue, usually during prolonged healing or inflammation. The resulting scar-like tissue can stiffen or distort normal tissue. Around an implant, fibrosis can increase the distance or electrical resistance between an electrode and nearby neurons.
Flicker fusion
Flicker fusion is the point at which a rapidly flickering light is perceived as steady. The corresponding critical flicker frequency depends on factors such as brightness, contrast, retinal location, and adaptation. It is used as a measure of temporal resolution in vision.
Food and Drug Administration (FDA)
The Food and Drug Administration (FDA) is a U.S. federal agency responsible for protecting public health by regulating products including medical devices, drugs, biological products, food, cosmetics, and radiation-emitting products. For bionic vision, the FDA oversees clinical investigations and reviews whether medical devices may be marketed in the United States.
Fovea
The fovea is a small specialized region at the center of the macula. It contains the retina's highest density of cone photoreceptors and supports the sharpest central vision and fine color discrimination. People direct their eyes so that objects of interest fall on the fovea.
Functional vision
Functional vision describes how a person uses their available sight in real-world activities, such as reading, recognizing objects, or navigating. It depends not only on visual acuity and visual field, but also on contrast, lighting, fatigue, familiarity, and the demands of the task.
Gene editing
Gene editing changes DNA at a chosen location in a cell's genome. It can be used to correct, disable, insert, or otherwise modify a genetic sequence. In inherited retinal disease, gene-editing strategies aim to address disease-causing variants, but delivery, specificity, durability, and safety remain important challenges.
Gene therapy
Gene therapy is a medical approach that treats or prevents disease by changing genetic material in a patient's cells. It may add a working gene, replace or silence a harmful gene, or edit a DNA sequence. In vision research, gene therapies are being developed for inherited retinal diseases caused by specific genetic variants.
Geographic atrophy (GA)
Geographic atrophy (GA) is an advanced form of dry age-related macular degeneration. It causes expanding areas of retinal pigment epithelium and photoreceptor loss, producing missing or blurred regions of vision that may eventually affect the center of the visual field. The term geographic refers to the patch-like appearance of the affected retinal areas.
Glaucoma
Glaucoma is a group of eye diseases that progressively damage the optic nerve. It is often associated with elevated pressure inside the eye, although damage can also occur at pressures considered normal. Peripheral vision is commonly affected first, and treatment with medication, laser procedures, or surgery can slow further loss but does not restore vision already lost.
Glutamate
Glutamate is the main excitatory neurotransmitter in the vertebrate nervous system. Neurons release it to activate glutamate receptors on other cells. In the retina, photoreceptors and bipolar cells use glutamate to transmit visual signals.
Hemianopia
Hemianopia, also called hemianopsia, is loss of vision in one half of the visual field. It usually results from damage along the visual pathways in the brain, such as after a stroke, rather than from damage to the eyes themselves. The pattern of loss depends on where the visual pathway is affected.
Histology
Histology is the study of the microscopic structure of tissues. Samples are typically fixed, sectioned, stained or labeled, and imaged to reveal cells and tissue organization. In implant studies, histology can be used to assess electrode placement, cell survival, inflammation, and fibrosis.
Humanitarian Device Exemption (HDE)
A Humanitarian Device Exemption (HDE) is an FDA marketing application for a device intended to treat or diagnose a disease or condition affecting no more than 8,000 people in the United States per year. Approval requires evidence that the device is reasonably safe and that its probable benefit outweighs its risks, but it is exempt from the usual requirement to demonstrate effectiveness. Use of the device generally requires institutional review board approval.
In silico
In silico describes experiments performed using computer models or simulations. These studies can test hypotheses, compare designs, or predict outcomes before or alongside laboratory and clinical experiments.
In vitro
In vitro describes experiments performed outside a living organism, usually with cells, tissue, or biological molecules in a controlled laboratory setting. In vitro studies allow precise manipulation but do not reproduce every interaction present in an intact organism.
In vivo
In vivo describes experiments or processes that occur within a living organism. These studies preserve interactions among tissues, circulation, immune responses, and behavior, but usually offer less experimental control than in vitro work.
Inflammation
Inflammation is the immune system's response to injury, infection, or irritation. It helps remove harmful material and begin repair, but persistent inflammation can damage tissue. Around an implant, inflammatory cells and signaling molecules can affect nearby neurons and device performance.
Instrumental activities of daily living (iADLs)
Instrumental activities of daily living (IADL) are more complex tasks that support independent living, such as shopping, preparing meals, managing medication and money, using communication devices, arranging transportation, and maintaining a household. They generally require more planning and interaction with the environment than basic activities of daily living.
Intracortical implant
An intracortical implant contains electrodes that penetrate into the cerebral cortex, placing recording or stimulation sites close to neurons. This proximity can provide relatively precise access to neural activity, but inserting electrodes into tissue can also produce injury and a foreign-body response.
see Blindness
Investigational Device Exemption (IDE)
An Investigational Device Exemption (IDE) allows an investigational medical device to be used in a clinical study to collect safety and effectiveness data. Studies involving significant-risk devices generally require an FDA-approved IDE as well as approval from an institutional review board before enrollment begins. An IDE permits clinical investigation; it is not authorization to market the device.
Late blind
Late blindness refers to blindness acquired after early childhood, after a person has had substantial visual experience. Previous vision may influence visual memories, spatial concepts, and adaptation to vision loss, but experiences and rehabilitation needs vary widely between individuals.
Lateral geniculate nucleus (LGN)
The lateral geniculate nucleus (LGN) is a paired structure in the thalamus that receives signals from retinal ganglion cells through the optic tract. It organizes and modulates this information before sending it through the optic radiations to primary visual cortex. The LGN also receives extensive feedback from the cortex and other brain regions.
Legally blind
Legal blindness is an administrative classification used to determine eligibility for certain services and benefits. In the United States, it generally means best-corrected visual acuity of 20/200 or worse in the better eye, or a visual field limited to 20 degrees or less in the better eye. A legally blind person may retain substantial usable vision, and definitions differ across countries and programs.
Light sensitivity
Legal blindness is an administrative classification used to determine eligibility for certain services and benefits. In the United States, it generally means best-corrected visual acuity of 20/200 or worse in the better eye, or a visual field limited to 20 degrees or less in the better eye. A legally blind person may retain substantial usable vision, and definitions differ across countries and programs.
Low vision
Low vision is reduced vision that cannot be fully corrected with ordinary glasses, contact lenses, medication, or surgery and that makes everyday tasks more difficult. It can involve central or peripheral vision loss, reduced contrast sensitivity, poor night vision, or other limitations. The term generally indicates that some useful vision remains, but its exact definition varies across clinical and community contexts.
Macula
The macula is the central region of the retina used for detailed, straight-ahead vision. It contains a high density of cone photoreceptors and includes the fovea at its center. Damage to the macula can impair reading, face recognition, and other tasks that depend on fine detail.
Macular degeneration
Macular degeneration is damage or deterioration of the macula, the central region of the retina used for detailed vision. It can cause distortion, blur, or missing areas in central vision while leaving peripheral vision relatively intact. Age-related macular degeneration is the most common form, but inherited and other macular disorders can produce similar effects.
see Action potential
Microelectrode array (MEA)
A microelectrode array (MEA) is a set of small electrodes arranged on a surface or penetrating structure. Each electrode can record electrical activity, deliver stimulation, or sometimes do both. In visual prostheses, the number, spacing, geometry, and placement of electrodes help determine which neurons can be addressed.
Nanoelectronic device
A nanoelectronic device is an electronic device that uses components, materials, or structures with dimensions measured in nanometers. Nanoscale features can enable very small sensors, electrodes, circuits, or light-sensitive elements. In bionic vision, nanoelectronic technologies may be used to increase device density, improve interfaces with cells, or reduce the size of implanted components.
National Institutes of Health (NIH)
The National Institutes of Health (NIH) is the primary U.S. federal agency supporting biomedical and public health research. It conducts research and funds work at universities, hospitals, and other institutions, including studies of vision, neuroscience, medical devices, and clinical care.
Neovascularization
Neovascularization is the growth of new blood vessels. It can be a normal part of healing, but in the eye abnormal vessels may be fragile, leaky, and disruptive to vision. Retinal or choroidal neovascularization occurs in several diseases, including diabetic retinopathy and some forms of macular degeneration.
Neurite
A neurite is a projection extending from the body of a neuron. The term includes developing or not-yet-classified axons and dendrites, and is often used when describing neurons grown in culture. Neurite length and branching are common measures of neural growth or damage.
Neuron
A neuron is a specialized cell that receives, processes, and transmits information in the nervous system. Neurons communicate through electrical signals within the cell and chemical or electrical signals at connections called synapses. Their shapes and response properties vary widely across the retina and brain.
Neuroprosthesis
A neuroprosthesis is a device that interfaces with the nervous system to restore, replace, or support a lost function. It may record neural activity, stimulate neural tissue, or do both. Visual prostheses, cochlear implants, and some brain-computer interfaces are examples of neuroprosthetic systems.
Neurorehabilitation
Neurorehabilitation is a form of rehabilitation for people affected by injury or disease of the brain, spinal cord, or peripheral nerves. It uses therapies, training, assistive technologies, and other interventions to help restore lost abilities, develop compensatory strategies, and improve independence and quality of life.
Occipital lobe
The occipital lobe is the rear portion of the cerebral cortex and contains most of the brain's visual areas. It receives and processes information about features such as location, orientation, motion, color, and shape before passing signals to other cortical regions.
Occipital seizure
An occipital seizure is a seizure that begins in the occipital lobe, the part of the brain containing most of the visual cortex. It may produce flashes, colors, shapes, temporary visual loss, or other visual disturbances. Electrical stimulation of visual cortex must be designed and monitored carefully because excessive stimulation can increase seizure risk.
Ophthalmology
Ophthalmology is the medical specialty concerned with the eyes, visual system, and related diseases. Ophthalmologists are physicians who diagnose and treat eye conditions using medication, laser procedures, surgery, rehabilitation referrals, and other forms of care.
Opsin
An opsin is a protein that responds to light when combined with a light-absorbing molecule or expressed as part of a light-sensitive system. Visual opsins in rods and cones initiate the biochemical signals that underlie normal vision. Other opsins are used in optogenetics to make selected cells respond to light.
Optic nerve
The optic nerve is formed by the axons of retinal ganglion cells and carries visual signals from each eye toward the brain. The two optic nerves meet at the optic chiasm, where some fibers cross before continuing in the optic tracts to targets including the lateral geniculate nucleus and superior colliculus. Damage to the optic nerve can cause permanent vision loss.
Optic nerve prosthesis
An optic nerve prosthesis is a device designed to create visual percepts by electrically stimulating the optic nerve. It bypasses damaged photoreceptors and retinal circuitry while relying on surviving nerve fibers to carry signals toward the brain. Because many visual signals are densely packed within the optic nerve, producing precise and interpretable percepts is technically challenging.
Optogenetics
Optogenetics uses genetic methods to make selected cells respond to light, usually by expressing light-sensitive proteins called opsins. Light can then increase or decrease the cells' electrical activity with precise timing. For sight restoration, researchers are studying whether surviving retinal neurons can be made light-sensitive after photoreceptors have been lost.
Orientation and Mobility (O&M)
Orientation and mobility (O&M) refers to the skills used to determine one’s position in an environment and travel safely and efficiently. O&M training for blind and low-vision people may involve sensory cues, remaining vision, a long cane, a guide dog, public transportation, or navigation technology. It is commonly provided by a trained orientation and mobility specialist.
Outcome measure
An outcome measure is a predefined observation or measurement used to evaluate a patient's health, function, or experience in a study. Examples include visual acuity, task performance, adverse events, or a patient-reported questionnaire. A clinical trial may use several outcome measures, with one designated as the primary outcome.
Partially sighted
Partially sighted is a broad term for someone who has reduced but not absent vision. It has been used in education, law, and rehabilitation, but has no single clinical definition and is less common in current United States usage. Many people prefer low vision, blind, or a more specific description of their vision.
Patch-clamp
Patch-clamp is an electrophysiology technique used to measure electrical currents or membrane voltage in individual cells. A fine glass pipette forms a tight seal with the cell membrane, allowing researchers to record from single ion channels or from the whole cell.
Perceptual learning
Perceptual learning is a lasting improvement in the ability to detect, distinguish, or interpret sensory information following experience or practice. In bionic vision, users may learn to interpret unfamiliar or degraded percepts produced by a prosthesis. Improvements may be specific to the trained task, stimulus, or visual location.
Peripheral vision
Peripheral vision is vision outside the central area of gaze. It is less sensitive to fine detail than central vision but is important for detecting motion, maintaining spatial awareness, and navigating through the environment. Some eye diseases primarily affect peripheral vision while initially preserving central acuity.
Phosphene
A phosphene is the phenomenon of seeing light without light actually entering the eye. Many patients have reported phosphenes as bright circular or streaky spots of light among darkness. Phosphenes can be directly induced by mechanical, electrical, or magnetic stimulation of the retina or visual cortex, or by random firing of cells in the visual system. Visual neuroprostheses have been found to stimulate phosphenes to restore vision to people with severe visual impairments. Most vision researchers believe that phosphenes result from the normal activity of the visual system after stimulation of one of its parts from some stimulus other than light.
Phosphene map
A phosphene map records where phosphenes appear and may also describe their shape, size, brightness, color, or stability. Researchers create these maps by stimulating individual electrodes or electrode combinations and collecting a person's perceptual reports. The map can be used to configure a prosthesis or study how stimulation relates to perception.
Photocurrent
Photocurrent is an electrical current generated or changed by exposure to light. It can arise in biological photoreceptors, light-sensitive proteins, or semiconductor devices such as photodiodes. Its size and timing help determine how strongly and quickly a system responds to light.
Photoreceptor
A photoreceptor is a specialized cell in the retina that detects light and begins the process of vision. Human photoreceptors are rods and cones, which contain light-sensitive opsins and signal to bipolar cells. Many retinal degenerative diseases damage photoreceptors while leaving some downstream retinal neurons intact.
Photoreceptor precursor
A photoreceptor precursor is an immature cell that has begun developing toward a rod or cone but is not yet fully mature. Such cells are studied as potential sources for replacing photoreceptors lost to retinal degeneration. They are more specialized than stem cells but may still require further development after transplantation.
Photovoltaic
Photovoltaic describes the direct conversion of light into electrical voltage or current by a material or device. Photovoltaic retinal implants can use light-sensitive pixels to generate electrical stimulation without a wired connection to each pixel.
Plasmid
A plasmid is a small DNA molecule that exists separately from the main chromosomes of a cell and can often reproduce independently. Scientists can engineer plasmids to carry selected genes into cells for research, manufacturing, or gene-delivery applications. Unlike viral vectors, plasmids do not use a modified virus to deliver their genetic material.
Pluripotent stem cell
A pluripotent stem cell can self-renew and develop into nearly any specialized cell type in the body. Embryonic stem cells and induced pluripotent stem cells are both pluripotent. In sight-restoration research, these cells can be guided toward retinal pigment epithelial cells, photoreceptors, or other retinal cell types for disease modeling or potential transplantation.
Primary visual cortex (V1)
Primary visual cortex, or V1, is the first major cortical stage of visual processing. It lies in the occipital lobe, receives organized input from the lateral geniculate nucleus, and contains a retinotopic map of the visual field. V1 neurons respond to features including position, orientation, contrast, and spatial frequency.
Psychophysical threshold
A psychophysical threshold is the stimulus level associated with a specified probability of detection or discrimination. For a phosphene, the detection threshold may be the minimum stimulation level that is perceived reliably. Because responses vary across trials, thresholds are usually estimated statistically rather than treated as perfectly sharp boundaries.
Psychophysics
Psychophysics is the study of the relationship between physical stimuli and the sensations, perceptions, or behavioral responses they produce. Common psychophysical methods measure detection thresholds, discrimination, perceived intensity, or task performance. In bionic vision, psychophysics is used to characterize electrically or optically evoked percepts and evaluate how useful they are.
Pulse width
Pulse width is the amount of time an individual stimulation pulse lasts, often measured in microseconds or milliseconds. Together with current amplitude, it helps determine the electric charge delivered in each pulse and which neural elements are activated.
Receptive field
A receptive field is the region of sensory space in which a stimulus can change a neuron's activity. For a visual neuron, it usually refers to a particular region of the visual field and the stimulus features that affect the cell. Receptive-field size and structure vary across the retina and visual brain.
Residual vision
Residual vision is the visual function a person retains after substantial vision loss. It may include light perception, motion detection, peripheral vision, or limited form vision. The term describes what vision remains but does not indicate whether it is useful for a particular task.
Retina
The retina is a thin layer of neural tissue lining the back of the eye. Photoreceptors convert light into biological signals, which are processed by retinal circuits and sent to the brain through the optic nerve. Many bionic-vision approaches stimulate surviving retinal neurons when photoreceptors have been lost.
Retinal degeneration
Retinal degeneration is the progressive dysfunction and death of retinal cells, often including rod and cone photoreceptors. It is not a single diagnosis but a process that occurs in conditions such as retinitis pigmentosa and age-related macular degeneration. The pattern, cause, and rate of cell loss vary between diseases.
Retinal detachment
Retinal detachment is the separation of the light-sensitive retina from the underlying tissue that supports it. This disrupts retinal function and can cause flashes, floaters, a shadow or curtain in the visual field, and vision loss. It requires prompt medical treatment to reduce the risk of permanent damage.
Retinal ganglion cell
A retinal ganglion cell (RGC) is an output neuron of the retina. It receives processed visual signals from bipolar and amacrine cells and converts them into action potentials. The axons of retinal ganglion cells leave the eye together to form the optic nerve and carry information to several brain regions.
Retinal pigment epithelium (RPE)
The retinal pigment epithelium (RPE) is a single layer of pigmented cells between the photoreceptors and the choroid. It supports photoreceptors by recycling visual molecules, removing shed material, regulating the local environment, and absorbing stray light. RPE dysfunction contributes to several retinal diseases and is a target of some cell therapies.
Retinal prosthesis
A retinal prosthesis is an implanted electronic device designed to create visual percepts by stimulating neurons that remain in a damaged retina. Visual information may come from an external camera or from light-sensitive components in the implant. Retinal prostheses are commonly classified by electrode location, including epiretinal, subretinal, and suprachoroidal designs.
Retinitis pigmentosa (RP)
Retinitis pigmentosa (RP) is a group of inherited retinal diseases in which photoreceptors progressively lose function and die. Rod loss commonly causes difficulty seeing at night and narrowing peripheral vision, followed in many forms by cone loss and reduced central vision. There is no single treatment for all forms of RP; vision rehabilitation and low-vision aids can help, while gene, cell, drug, and prosthetic approaches are under study.
Retinotopy
Retinotopy is the orderly mapping of the visual field onto neural tissue. Nearby points in visual space are generally represented by nearby cells in the retina and in several visual brain areas. Visual prostheses often rely on retinotopy to choose where stimulation should produce a percept.
Rod photoreceptor
A rod photoreceptor is a retinal cell specialized for vision in dim light. Rods are highly sensitive but do not support color vision and are most numerous outside the fovea. In many forms of retinitis pigmentosa, rod dysfunction and loss occur before cone degeneration.
Secondary visual cortex (V2)
Secondary visual cortex, or V2, is a visual area next to V1 in the occipital lobe. It receives strong input from V1 and sends information to several higher visual areas. V2 contributes to processing contours, depth, figure-ground organization, and other aspects of visual form.
Sensory substitution
Sensory substitution converts information normally obtained through one sense into signals delivered through another. For example, a camera image may be translated into sound or patterns of touch for a blind user. The system does not directly restore retinal function, but training can help users interpret the substituted signals for practical tasks.
Simulated prosthetic vision (SPV)
Simulated prosthetic vision (SPV) is a computer-generated approximation of what a visual prosthesis might produce. It is commonly shown to sighted participants in a display or virtual-reality system to evaluate image-processing strategies, task performance, or device designs before or alongside implant studies. SPV is a model and may not capture the full appearance or variability of real electrically evoked percepts.
Spatial frequency
Spatial frequency describes how often a visual pattern repeats across space. It is commonly measured in cycles per degree of visual angle. Low spatial frequencies represent broad, coarse structure, while high spatial frequencies represent fine detail.
Spiking neural network (SNN)
A spiking neural network (SNN) is a computational model in which artificial neurons communicate using discrete events called spikes. Unlike conventional neural networks, spiking models explicitly represent the timing of neural activity. They are often used to study biological neural systems or to develop energy-efficient computing systems inspired by the brain.
Stem cell
A stem cell can produce more stem cells and develop into one or more specialized cell types. Researchers can guide some stem cells toward retinal cells for disease modeling, drug testing, or potential transplantation. Different stem-cell types vary in where they come from and which cell types they can become.
Stimulation frequency
Stimulation frequency is the number of stimulation pulses delivered per unit time, usually measured in hertz. Changing frequency can alter perceived brightness, temporal continuity, adaptation, and neural recruitment. Its effects depend on the pulse waveform, amplitude, electrode location, and neural tissue being stimulated.
Subretinal
Subretinal means located beneath the neural retina, in the space between the photoreceptors and the retinal pigment epithelium. Subretinal prostheses stimulate surviving retinal cells from this position and may use light-sensitive pixels that respond to images projected onto the retina.
Suprachoroidal
Suprachoroidal means located between the choroid, a vascular layer behind the retina, and the sclera, the outer wall of the eye. Placing a prosthesis in this space can offer surgical stability and reduce direct contact with the retina, although the electrodes are farther from retinal neurons.
Thalamic visual prosthesis
A thalamic visual prosthesis is a device intended to create visual percepts by stimulating a visual structure in the thalamus, usually the lateral geniculate nucleus. This approach bypasses the eyes and optic nerves while targeting a region that contains an organized map of the visual field. It remains less extensively studied than retinal and cortical prostheses.
Total blindness
Total blindness means having no light perception. It is much narrower than blindness in general, because many people who are blind retain some visual perception or usable vision. The term describes a level of visual function, not a person’s independence or abilities.
Transcutaneous connector
A transcutaneous connector passes through the skin to provide a direct electrical connection between an implanted device and external equipment. It can transmit power, stimulation commands, or recorded signals without relying on a wireless link. Because it creates a permanent opening through the skin, it can increase the risk of infection and requires careful maintenance.
Viral vector
A viral vector is a virus modified to carry genetic material into selected cells. Vectors used in gene therapy are engineered to reduce or remove their ability to cause disease while retaining their delivery machinery. The choice of vector affects which cells are reached, how much genetic material can be carried, and how long expression may last.
Vision loss
Vision loss is a broad term for a partial or complete reduction in sight. It may be mild or severe, temporary or permanent, and caused by changes in the eyes, visual pathways, or brain. The term does not by itself indicate a particular diagnosis, level of function, or legal classification.
Visual acuity
Visual acuity is the ability to distinguish fine spatial detail, usually measured with a letter or symbol chart. A value such as 20/70 means that a person at 20 feet can resolve detail that a person with 20/20 acuity can resolve at 70 feet. Acuity primarily measures central detail vision and does not capture visual field, contrast sensitivity, or performance in everyday tasks.
Visual angle
Visual angle is the angle an object or pattern subtends at the eye. It depends on both physical size and viewing distance and is usually measured in degrees, minutes, or seconds of arc. Expressing size in visual angle allows visual stimuli to be compared across different displays and viewing distances.
Visual field
The visual field is the area that can be seen while the eyes remain directed at a fixed point. It includes central and peripheral vision. Visual-field testing measures the location and sensitivity of vision across this area and can reveal loss caused by retinal, optic-nerve, or brain disorders.
Visual function
Visual function refers to measurable aspects of vision, such as visual acuity, visual field, contrast sensitivity, color vision, and light sensitivity. It describes what the visual system can detect or discriminate under specified testing conditions. This differs from functional vision, which describes how a person uses their available vision in everyday activities.
Visual impairment
Visual impairment is an umbrella term for reduced visual function, including low vision and blindness. In clinical and research settings, it may be defined using visual acuity, visual field, contrast sensitivity, or other measures. It is broader than low vision and different from legal blindness, which is an administrative classification. Although visual impairment remains common in medicine and research, some Blind people and advocacy organizations prefer blind, low vision, or blind and low vision. When referring to a person, their own choice of language should take precedence.
Visual prosthesis
A visual prosthesis is a device intended to create visual percepts by stimulating part of the visual system. Depending on the design, electrodes may target the retina, optic nerve, thalamus, or visual cortex. The goal is usually to provide limited but useful visual information rather than reproduce normal vision.
A
B
C
D
E
F
G
H
I
L
M
N
O
P
R
S
T
V
Quick Links
Contact Us
This is a community project. Find out more about our team of contributors. If you'd like to contribute, please contact us.
Media Copyright Information
All images used with permission. Introduction graphic: © Getty. Background graphic: © Tracy Spohn/Shutterstock.
Made with at UC Santa Barbara, with generous support from the bionic vision community (2020—2026).
 All our content (unless otherwise noted) is licensed under CC-BY 4.0.
All our content (unless otherwise noted) is licensed under CC-BY 4.0.